Endocrine-disrupting chemicals are not a niche issue. They are a modern public-health issue.
The science is now substantial: hormone-disrupting exposures are widespread, biologically plausible, often continuous, and especially relevant during sensitive windows such as pregnancy, infancy, childhood, and puberty.
This page is designed to help clinicians quickly understand why endocrine-disrupting chemicals deserve serious public-health attention — not because every outcome is fully settled, but because the combination of widespread exposure, endocrine vulnerability, mixture effects, and delayed clinical consequences creates a problem that standard toxicology and routine clinical training have often underestimated.
Why EDCs matter beyond individual product choices
Endocrine-disrupting chemicals matter at population scale because hormones regulate development, metabolism, reproduction, thyroid signaling, stress physiology, and tissue maintenance at extremely low concentrations. This means biologically meaningful disruption can occur in ways that are easy to miss if the wrong endpoints, the wrong timing, or the wrong study designs are used.
Exposure is widespread and comes from many small sources at once: food contact materials, household dust, water, personal care products, occupational settings, and consumer goods.
People are exposed to mixtures, not one chemical at a time. Small contributions can accumulate into a larger endocrine burden.
Timing matters. Exposure during fetal life, infancy, childhood, puberty, and preconception may shape risk trajectories years later.
Some chemicals persist and bioaccumulate; others are cleared more quickly but are replenished by repeated everyday contact.
The burden is uneven. Vulnerability is shaped by occupation, housing, income, geography, and life stage.
Taken together, these features turn endocrine disruption into a public-health problem rather than a purely individual or consumer-choice issue.
Eight reasons endocrine disruption is difficult to ignore
These pillars explain why clinicians increasingly encounter EDC-related questions in reproductive medicine, thyroid practice, pediatrics, metabolic care, public health, and prevention-focused counselling.
Broad endocrine interference
Disruption is not limited to receptor mimicry. Chemicals may affect synthesis, secretion, transport, metabolism, receptor signaling, and downstream gene expression.
Chronic background exposure
Contact is frequent, repeated, and often invisible in daily life.
Mixtures and cumulative load
Combined exposure can matter even when individual chemicals appear modest in isolation.
Critical windows and latency
Early-life exposure can shape outcomes that emerge much later.
Networked physiology
Reproductive, thyroid, metabolic, developmental, and stress axes interact rather than operating in isolation.
Persistence versus replenishment
Both long-lived body burdens and repeated short-lived exposure patterns can sustain endocrine relevance.
Evidence triangulation
Mechanistic data, animal studies, and human observational research often converge even when no single study is definitive on its own.
Regulatory mismatch
Conventional hazard testing may miss low-dose, timing-specific, tissue-specific, and endocrine-relevant endpoints.
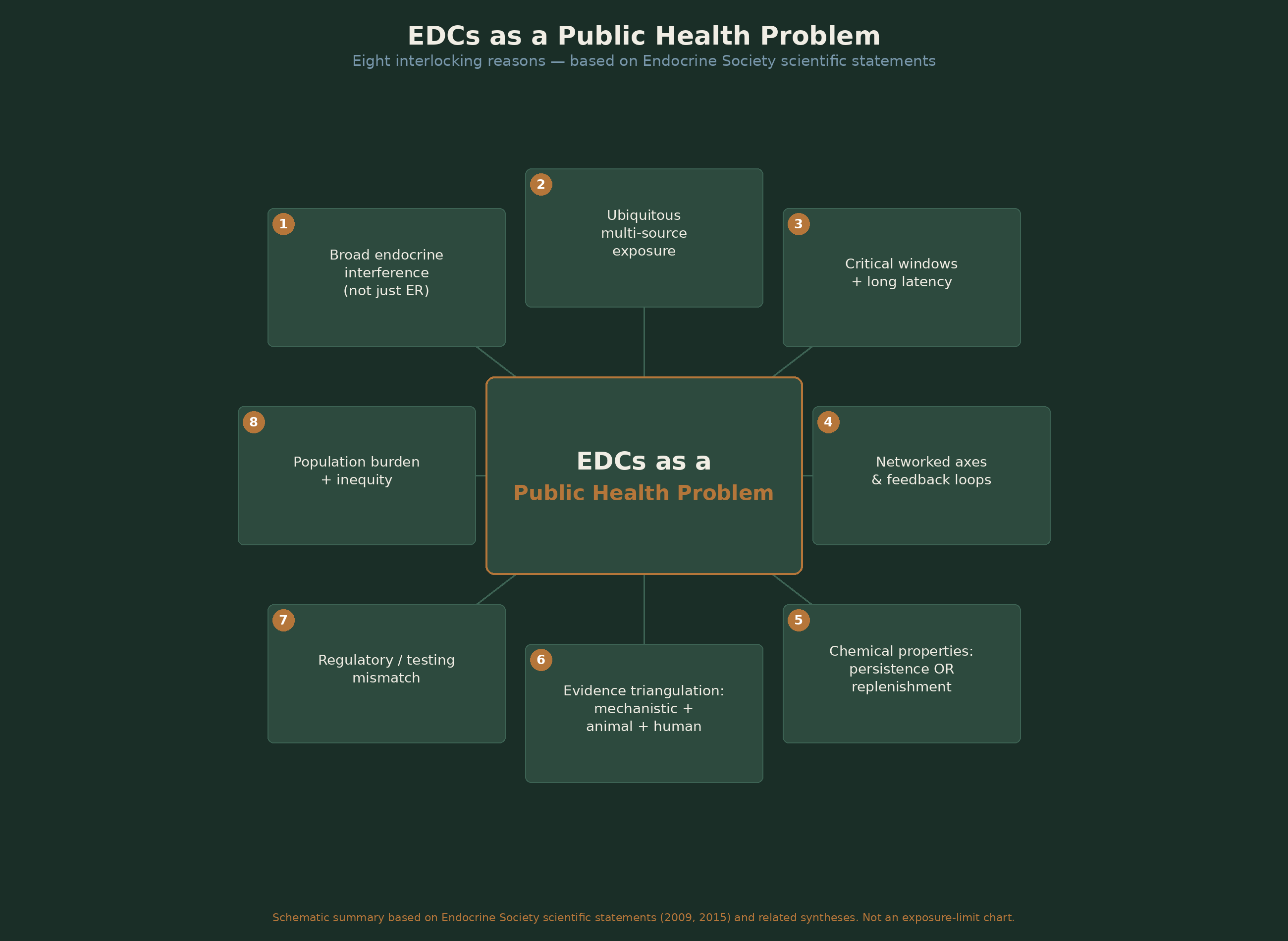
Schematic summary based on Endocrine Society scientific statements (2009, 2015) and related syntheses. Not an exposure-limit chart.
Why one simple rule does not work for all endocrine disruptors
“EDCs” is an umbrella term, not a single mechanism. PFAS, bisphenols, phthalates, flame retardants, pesticides, and related chemical families differ in persistence, tissue distribution, route of exposure, endocrine targets, and the life stages during which they are most relevant.
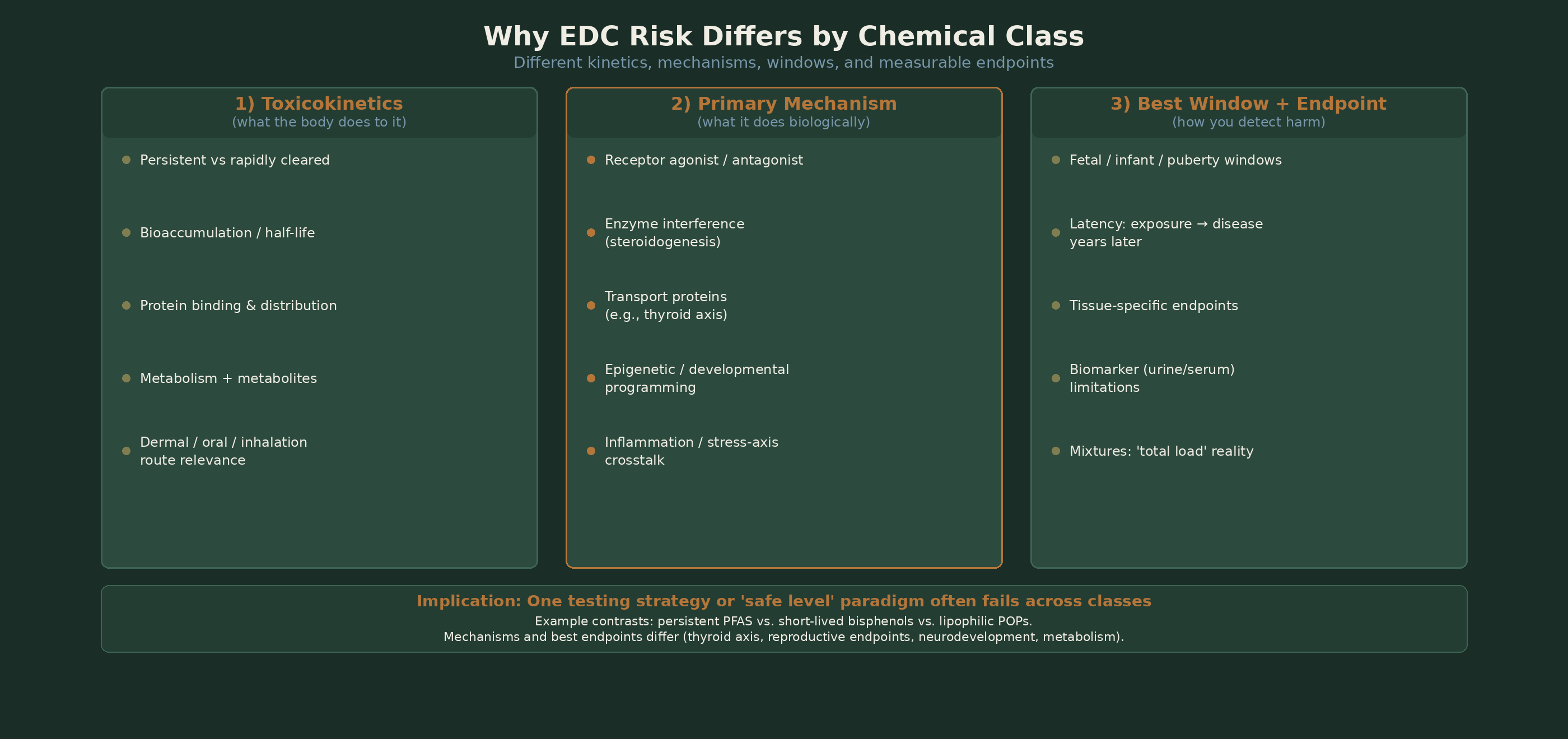
Different kinetics, mechanisms, windows, and measurable endpoints — one testing strategy or 'safe level' paradigm often fails across classes.
For clinicians, the practical implication is simple: avoid oversimplified messaging. The most useful framework is total load, sensitive windows, and feasible risk reduction.
Why this belongs in a consultation room
Patients increasingly ask whether environmental exposures may be relevant to fertility, thyroid function, metabolic health, cancer risk, pregnancy, or child development.
Clinicians do not need perfect causal certainty for every chemical-endpoint pair to justify low-risk exposure reduction advice, especially during sensitive windows.
A public-health framing helps clinicians avoid two common errors: dismissing the issue entirely or overstating certainty beyond the evidence.
The useful middle ground is evidence-based precaution: acknowledge uncertainty honestly, recognize where the science is already strong enough to warrant concern, and prioritize realistic interventions with low downside.
From public-health framing to clinical relevance
The broader public-health case is the foundation. Clinical decision-making begins when that foundation is translated into specific domains such as fertility, ovarian reserve, feminine-care exposures, thyroid vulnerability, pregnancy, childhood, and patient counselling.
For a focused example of how endocrine-disruptor science intersects with clinical care, continue to the EDCs & Feminine Health primer. That page gives a more applied overview of the evidence linking EDCs with female reproductive and fertility-related outcomes, while maintaining careful language around strength of evidence and causality.
Key References
- 1.Diamanti-Kandarakis E, Bourguignon JP, Giudice LC, et al. Endocrine-disrupting chemicals: an Endocrine Society scientific statement. Endocr Rev. 2009;30(4):293–342. PubMed: 19502515. PMC full text available.
- 2.Gore AC, Chappell VA, Fenton SE, et al. EDC-2: The Endocrine Society’s second scientific statement on endocrine-disrupting chemicals. Endocr Rev. 2015;36(6):E1–E150.
- 3.WHO / UNEP. State of the Science of Endocrine Disrupting Chemicals. 2013.
- 4.Endocrine Society. Introduction to endocrine-disrupting chemicals. Topic hub and educational materials.
- 5.Trasande L, et al. Estimating burden and disease costs of exposure to endocrine-disrupting chemicals in the European Union. Lancet Diabetes Endocrinol. 2016.
- 6.Vandenberg LN, Colborn T, Hayes TB, et al. Hormones and endocrine-disrupting chemicals: low-dose effects and nonmonotonic dose responses. Endocr Rev. 2012.